Article Text

Abstract
Background Hand, foot and mouth disease (HFMD) affects millions of children across Asia annually, leading to an increase in implemented control policies such as surveillance, isolation and social distancing in affected jurisdictions. However, limited knowledge of disease burden and severity causes difficulty in policy optimisation as the associated economic cost cannot be easily estimated. We use a data synthesis approach to provide a comprehensive picture of HFMD disease burden, estimating infection risk, symptomatic rates, the risk of complications and death, and overall disability-adjusted life-year (DALY) losses, along with associated uncertainties.
Methods Complementary data from a variety of sources were synthesised with mathematical models to obtain estimates of severity of HFMD. This includes serological and other data extracted through a systematic review of HFMD epidemiology previously published by the authors, and laboratory investigations and sentinel reports from Singapore’s surveillance system.
Results HFMD is estimated to cause 96 900 (95% CI 40 600 to 259 000) age-weighted DALYs per annum in eight high-burden countries in East and Southeast Asia, with the majority of DALYs attributed to years of life lost. The symptomatic case hospitalisation rate of HFMD is 6% (2.8%–14.9%), of which 18.7% (6.7%–31.5%) are expected to develop complications. 5% (2.9%–7.4%) of such cases are fatal, bringing the overall case fatality ratio to be 52.3 (24.4–92.7) per 100 000 symptomatic infections. In contrast, the EV-A71 case fatality ratio is estimated to be at least 229.7 (75.4–672.1) per 100 000 symptomatic cases. Asymptomatic rate for EV-A71 is 71.4% (68.3%–74.3%) for ages 1–4, the years of greatest incidence.
Conclusion Despite the high incidence rate of HFMD, total DALY due to HFMD is limited in comparison to other endemic diseases in the region, such as dengue and upper respiratory tract infection. With the majority of DALY caused by years of life lost, it is possible to mitigate most with increased EV-A71 vaccine coverage.
- Mathematical Modelling
- Epidemiology
- Paediatrics
- Other Infection, Disease, Disorder, Or Injury
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Hand, foot and mouth disease (HFMD) is a high-incidence paediatric disease with notified cases exceeding a million each year. Although the number of mild cases vastly outnumbers severe cases, the potential for complications and death has led to an inflated perception of disease severity, which incited a stronger response than necessary in multiple jurisdictions in Asia.
Although the symptomatic case fatality rate (sCFR) of HFMD has been computed in the literature, it is a poor reflection of the general severity and disease burden because it is sensitive to the notification rates of the surveillance system.
What are the new findings?
Using a combination of Singapore’s surveillance data along with serological and epidemiological data found in the literature, we constructed a series of models and indices that describe the entire spectrum of HFMD severity. These findings were translated into an age-weighted disability-adjusted life-years (DALY) for comparison to other diseases.
Our results show that after correcting for non-notification sCFR is likely to be inflated many times. Also, disability plays a minor part in overall DALY and the majority of DALYs could be lowered if fatality rate is lowered, possibly with the EV-A71 vaccine. High asymptomatic rates have profound implications to the modelling studies previously conducted to estimate the reproduction number of EV-A71, which have been generally heterogeneous.
Recommendations for policy
Policies directed at HFMD should be re-evaluated based on this updated estimate of disease severity and burden.
Introduction
Hand, foot and mouth disease (HFMD) is a paediatric disease which, although usually self-limiting, can result in complications associated with the central nervous system (CNS) or death.1 2 The viruses that cause HFMD are particularly widespread in Asia, where they are responsible for millions of infections each year.3 An outbreak in Malaysia between April and June 1997 in which 29 children died4 was a harbinger of fatal outbreaks that have continued to recent years (170 deaths in Vietnam in 20115 and 98 deaths in Cambodia in 2012).6 These fatal outbreaks have influenced the perceived severity of HFMD and led to the demand for control measures,7 such as the recent phase III vaccine trials in China,8 despite the limited information on the disease burden. Many affected countries, such as China, Japan and Singapore, adopted routine control measures akin to those from pandemic preparedness plans—including surveillance, mandatory reporting, isolation, school closures and social distancing—but optimal use of such interventions requires the disease burden of HFMD to be quantified so that the public health response can be calibrated accordingly.
The main aetiological agents of HFMD are the human enterovirus A71 (EV-A71) and coxsackieviruses 10 and 16, with EV-A71 being associated with more severe outcomes. As with other usually mild diseases where infections vastly exceed severe cases, efforts to track all HFMD infections to determine indices for different levels of severity are impractical due to the large number of cases involved.9 With the exception of a few jurisdictions, much of the data on HFMD are based on subpopulations, such as the catchment of a health system, a network of sentinel clinics or from passive surveillance using symptomatic case notifications (for instance, ref 10). Such studies may provide an incomplete view of the true burden of disease. Obtaining a more comprehensive picture requires synthesising available information from studies across all severity levels, from serological studies that estimate infection risk, to notification data that provide information on symptomatic cases that could be clinically identified, to hospital records that showcase the risk of more severe expressions such as CNS complications or death. Such estimates need to be constructed carefully to allow uncertainty to be properly reflected and accounted for. This can be achieved through Bayesian methods which provide a flexible framework to integrate data from multiple sources and have been used to estimate infection rates and severity indices for influenza11 12 and HIV.13
To quantify the extent of HFMD across Asia, its mortality risk and the economic burden of control measures against it,7 we conducted an analysis using data from a previous systematic review of research across East and Southeast Asia14 to develop estimates of disease burden at different levels of severity. Specifically, we adopted a modelling approach that combined serological surveys, epidemiological studies and surveillance data to estimate the risk of children being infected, symptomatic, hospitalised, afflicted with complications and dying. These estimates and the age-weighted method15 were used to derive estimates of disability-adjusted life-years (DALY) lost across Asia due to HFMD.
Methods
The severity of infection was classified into tiers which require different levels of care: (i) clinically apparent, or symptomatic, cases; (ii) hospitalisations; (iii) complications, or severe cases when the child displays neurological or cardiopulmonary complications; and (iv) fatal cases. These manifestations were matched against similar definitions from the Global Burden of Disease 2013 (GBD2013) study16 that have existing estimates of disability weights, and the overall disease burden is the average of each level of severity, weighted by the proportion of cases entering into each level.
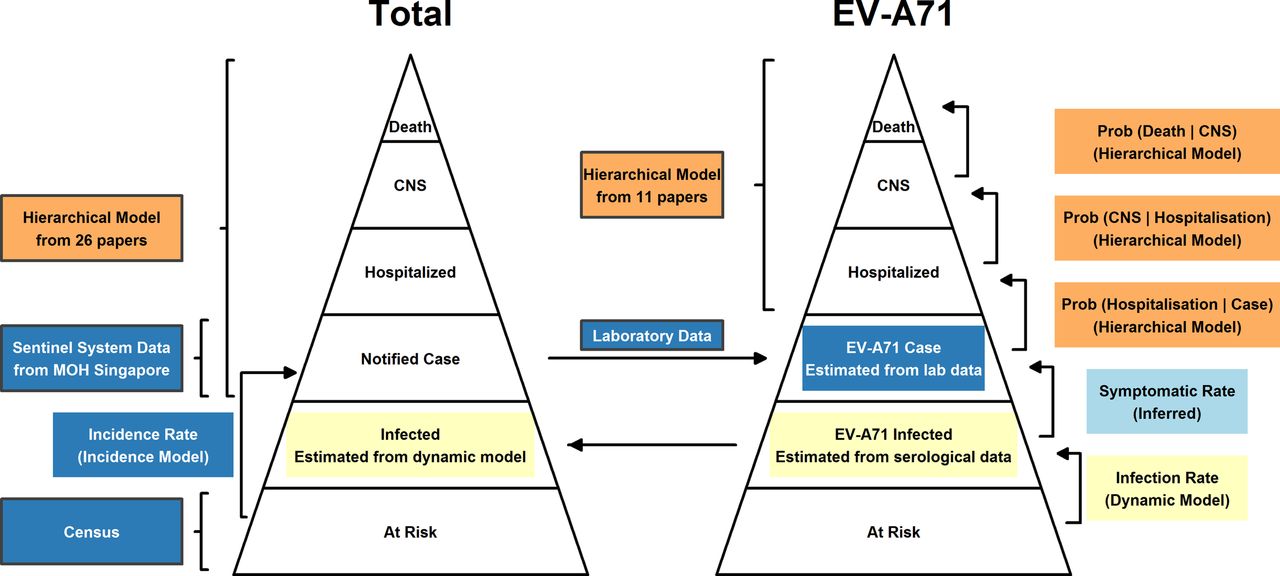
These severity tiers were arranged as a pyramid where lower echelons represent the majority of (milder) infections with decreasing frequency but increasing severity towards the apex11 17 (figure 1). The parameters which describe the severity of HFMD are the proportions of individuals in one state who reach the next higher severity level. This framework implicitly assumes that cases with higher severity are a proportion of cases at the preceding level. For example, those with significant CNS complications are modelled to be a subset of hospitalised cases, and similarly, all hospitalised cases are a subset of notified cases. We built two parallel pyramids for total HFMD (of all aetiologies) and specifically for EV-A71 due to the abundance of data on EV-A71 compared with other viruses, as well as this virus being thought to be responsible for more severe symptoms.

The severity pyramid structure for hand, foot and mouth disease (HFMD) (total, all aetiologies) and EV-A71 in particular. Bordered boxes are data sources, while boxes within the pyramids are estimated quantities. Pale yellow boxes represent the models and outcomes of submodel 1, the infection rate model. This model uses serological data and differential equations to estimate the rate at which infection must occur to match with observed seropositivity level of EV-A71. Blue boxes represent the data, model and outcomes of submodel 2, the symptomatic incidence rate model. This model uses surveillance data from Singapore to infer the incidence rate of HFMD and EV-A71-specific HFMD. Together with submodel 1, the estimated symptomatic rate of EVA71 (cyan box) can be calculated. The orange boxes represent the data and models of submodel 3: the hierarchical model, which is used to estimate indices that quantifies the higher-level severities of HFMD. CNS, central nervous system; MOH, Ministry of Health.
Quantifying the disease burden of HFMD requires an estimate of the total number of cases, which was calculated from the infection rate (both symptomatic and asymptomatic) obtained from seroepidemiological studies. From a systematic review previously published by the authors,14 we extracted 10 studies of EV-A71 serology18–28 (online supplementary appendix A1, A2 and A3) from which the seropositive rate of EV-A71 by age was found using submodel 1 to model the required infection rate to achieve the observed seroprevalence.
Supplementary file 1
To estimate clinically apparent cases, we used data on notified cases from Singapore, where HFMD is a legally notifiable disease and where active surveillance in preschools is conducted via daily temperature taking; this was used to calculate a lower bound for the overall asymptomatic rate of HFMD, in submodel 2. Indices for higher severity levels of HFMD and EV-A71, which include deaths, complications, hospitalisations and symptomatic cases, used information from 27 papers5 29–54 and 11 papers29 34 35 39 55–61 respectively from across Asia and were modelled in submodel 3. Finally, the severity indices estimated in the three submodels were fused to collectively estimate the overall disease burden of HFMD in Asia.
Submodel 1: infection rate model
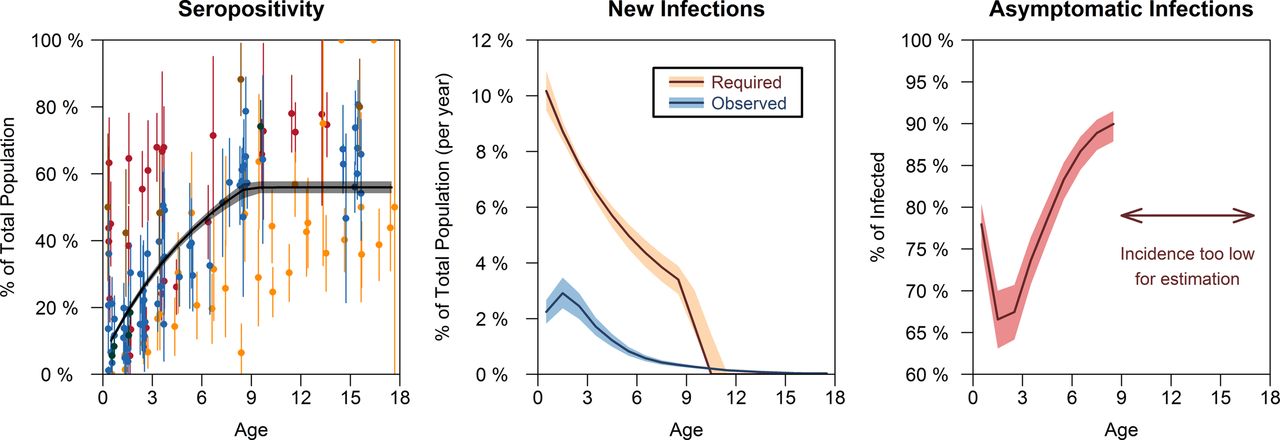
The infection rate model estimates the age-specific proportion of children who must be infected by the EV-A71 virus each year to reach the observed level of seroprevalence. Serological data from China,18–20 Singapore,21 22 Taiwan,23 24 26 Thailand27 and Vietnam28 were extracted from the original papers (figure 2, left), from which it can be observed that seropositivity to EV-A71 starts low at infancy and reaches a plateau around 40%–60% by adolescence, a finding which is corroborated by cord blood seropositivity (indicative of maternal antibody levels) of 55% in Vietnam,28 47%–50% in Taiwan,25 26 38% in Singapore21 and 26% in China.62 To accommodate these patterns, we developed and fit models of the age-specific seroprevalence using seven dynamical models which make varying assumptions for the reason behind these phenomena. These assumptions include (i) an infection rate that drops to zero at age T, beyond which no further infection is possible; (ii) an exponentially decreasing infection rate which is asymptotically zero as age increases and (iii) antibodies for EV-A71 in humans will diminish over time like influenza63 64 and eventually reach an equilibrium from new infections and loss of immunity. The details of each of the models are explained further in online supplementary appendix A1.
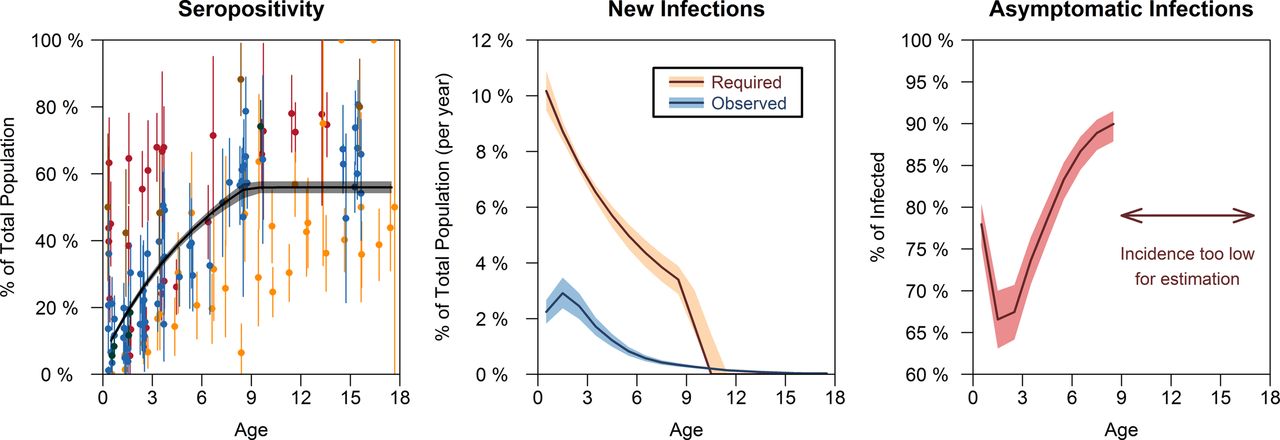
Data and results from the infection rate model (submodel 1). Left: seropositivity levels of EV-A71 with fitted curve. Red data points are from China, blue from Taiwan and orange from Singapore, green from Vietnam and brown from Thailand. The black line is the fitted model with 95% Bayesian credible intervals. Middle: required and observed rate of EV-A71 infection. The brown line shows the age-specific infection rate of EV-A71 implied from the seropositivity curve and is the required rate to get the observed seropositivity levels; the blue line shows the calculated average EV-A71 infection rate based on Singapore’s data from submodel 2. The difference between the two lines are the unobserved cases. Right: asymptomatic infection rate. Calculated from the percentage difference between the required and observed rates of infection in the middle.
Posterior distributions of parameters were estimated in R65 using Markov chain Monte Carlo (MCMC) and R package ‘deSolve’66 with non-informative prior distributions. The optimal model to represent infection rate was determined by the fit to the data and the model complexity and was evaluated using the deviance information criteria (DIC).
Submodel 2: symptomatic incidence rate model
Since October 2000, Singapore has adopted a comprehensive approach for HFMD surveillance including a mandatory case reporting system by medical practitioners and childcare centres,67 with children at childcares being screened once or twice daily for symptoms and then subsequently isolated for 10 days if symptomatic. The clearly defined population catchment in the city-state and the dual layers of doctor-driven and teacher-driven surveillance make the data on notified symptomatic presentations of HFMD collected by the Singapore’s Ministry of Health unusually complete compared with the rest of Asia. In calculating symptomatic incidence rate, we make the assumption that all symptomatic paediatric HFMD were clinically apparent and captured by the surveillance system in Singapore.
We constructed a matrix containing the incidence  of cases in year
of cases in year  (2003–2012) among age a (1–18), scaled by the number of individuals in the resident population for that age and year derived from the census.68 To separate the effects of age and time on incidence rate, singular value decomposition was performed on the incidence matrix to find the first left-singular vector
(2003–2012) among age a (1–18), scaled by the number of individuals in the resident population for that age and year derived from the census.68 To separate the effects of age and time on incidence rate, singular value decomposition was performed on the incidence matrix to find the first left-singular vector  which corresponds to the largest singular value. This vector is normalised to
which corresponds to the largest singular value. This vector is normalised to  , which is equivalently the normalised first principal component of
, which is equivalently the normalised first principal component of  , and represents the systematic variation attributable to age. The second vector is a time-series index,
, and represents the systematic variation attributable to age. The second vector is a time-series index,  , representing the stochastic variation attributable to HFMD incidence level each year. Values for years 2013–2015 were estimated using linear regression using data from Singapore’s Weekly Infectious Disease Bulletin.69 The modelled HFMD incidence rate is estimated from the product of the two vectors,
, representing the stochastic variation attributable to HFMD incidence level each year. Values for years 2013–2015 were estimated using linear regression using data from Singapore’s Weekly Infectious Disease Bulletin.69 The modelled HFMD incidence rate is estimated from the product of the two vectors,  .
.
The EV-A71-specific incidence is a proportion of all HFMD cases. We obtain  , the year effect due to EV-A71, by taking it as a binomial sample from the total year effect,
, the year effect due to EV-A71, by taking it as a binomial sample from the total year effect,  . The proportion of cases attributed to EV-A71 in 2008–2015,
. The proportion of cases attributed to EV-A71 in 2008–2015,  , was estimated from data obtained from the National Surveillance Program in Singapore which collects clinical specimens from patients in 107 clinics and 2 hospitals, KK Women’s and Children’s Hospital and National University Hospital (figure 3, right). Throat or vesicle swabs were collected from patients <12 years of age with clinical diagnosis of HFMD. Specimens were stored at room temperature or 4° (preferred) for no longer than 48 hours, before being sent to the National Public Health Laboratory for testing and typing. Data on
, was estimated from data obtained from the National Surveillance Program in Singapore which collects clinical specimens from patients in 107 clinics and 2 hospitals, KK Women’s and Children’s Hospital and National University Hospital (figure 3, right). Throat or vesicle swabs were collected from patients <12 years of age with clinical diagnosis of HFMD. Specimens were stored at room temperature or 4° (preferred) for no longer than 48 hours, before being sent to the National Public Health Laboratory for testing and typing. Data on  prior to 2008 were estimated in a study by Ang et al.52 The average EV-A71 incidence rate by age is the average of the EV-A71 year effect, weighted by the age effect, or
prior to 2008 were estimated in a study by Ang et al.52 The average EV-A71 incidence rate by age is the average of the EV-A71 year effect, weighted by the age effect, or  . The model is described in detail in online supplementary appendix B.
. The model is described in detail in online supplementary appendix B.

Age and year trend of hand, foot and mouth disease (HFMD) symptomatic infection from the Incidence rate model (submodel 2). Left: the age effect. The black line reflects the overall proportion of incidence for each year of age, and red line represents the age effect for individual years from 2005 to 2012. Middle: the year effect. The black line is an index which reflects the number of notified cases for 2005–2012. The year effect for 2013–2015 is estimated from data (notified cases) obtained from the Weekly Infectious Disease Bulletin released by the Ministry of Health, Singapore, using linear regression. The year effect of EV-A71 (blue) is mathematically derived from the proportion of cases due to EV-A71 estimated by laboratory data (right). Right: laboratory data from Singapore’s surveillance system. This shows the proportion of cases due to each virus in each year from 2005 to 2015.
Submodel 3: hierarchical model of disease severity
The upper levels of the severity pyramid from across Asia were modelled as nested binomial distributions, with the probability of reaching state i or higher given the case reaches the lower state j denoted as  . The states are D (death), S (severe disease, ‘CNS’), H (hospitalised) and C (symptomatic case) so that, for example,
. The states are D (death), S (severe disease, ‘CNS’), H (hospitalised) and C (symptomatic case) so that, for example,  denotes the case hospitalisation rate. Standard rules of conditional probability mean that the product of these probabilities gives the risk of progressing through multiple levels; for instance, the overall case fatality rate (CFR) is
denotes the case hospitalisation rate. Standard rules of conditional probability mean that the product of these probabilities gives the risk of progressing through multiple levels; for instance, the overall case fatality rate (CFR) is  . As a result, the likelihood function for data with missing tiers of the pyramid is specified via combinations of the basic parameters. For example, 4625 hospitalisations and 11 deaths were documented in the Sarawak 1997 outbreak,49 with no mention of severe cases. This data set will allow us to estimate
. As a result, the likelihood function for data with missing tiers of the pyramid is specified via combinations of the basic parameters. For example, 4625 hospitalisations and 11 deaths were documented in the Sarawak 1997 outbreak,49 with no mention of severe cases. This data set will allow us to estimate  , and thus make inferences on
, and thus make inferences on  and
and  through the multiplicative relationship, where
through the multiplicative relationship, where  is the individual-level estimate for paper p. Detailed description of the model and all data sources can be found in online supplementary appendix C1 (data), C2 and C3 (results) and C4 (model). The posterior distribution of parameters were estimated using the Metropolis Hastings algorithm (MCMC) in R.
is the individual-level estimate for paper p. Detailed description of the model and all data sources can be found in online supplementary appendix C1 (data), C2 and C3 (results) and C4 (model). The posterior distribution of parameters were estimated using the Metropolis Hastings algorithm (MCMC) in R.
Disability-adjusted life-year burden
To estimate the DALY lost across Asia to HFMD, we conservatively estimated the incidence of HFMD infection to be twice the incidence of EV-A71 using the incidence rate model (submodel 2), to allow for infection by other aetiological agents of HFMD which tend to be more common than EV-A71. The number of symptomatic cases was then calculated using the asymptomatic rate from the infection rate model (submodel 1). The numbers of more severe manifestations (hospitalised, CNS and deaths) were then estimated using the parameters from the hierarchical model (submodel 3). Again, posterior distributions were used to characterise uncertainty in these estimates.
Disability weights from GBD201316 for severe (0.133, 0.088–0.19), moderate (0.051, 0.032–0.074) and mild (0.006, 0.002–0.012) acute episodes of infectious disease were used as estimates for HFMD with complication, hospitalisation and symptomatic HFMD, respectively. To estimate the disability duration of each tier, we extracted commonly reported summary statistics such as the sample size, mean, median, range, CIs and variances of the disability duration of their samples from 31 papers and modelled them into Weibull distributions which best describe the statistical properties (online supplementary appendix D). The disability duration for fatalities was determined using the period life expectancy of Japan,70 which represents the expected lifespan of humans as healthcare improves in the current century.
We used the age-weighted approach15 which assigns greater weights to illnesses that occur during periods when the social role is higher, most notably between ages 10 and 55. As disability from HFMD usually occurs among children, this method provides a conservative estimate of DALY.
Under this framework, the formula for DALY for an individual is

where  is the disability weight (1 for premature mortality),
is the disability weight (1 for premature mortality),  =0.03 is the discount rate,
=0.03 is the discount rate,  =0.166 is the age-weighting correcting coefficient,
=0.166 is the age-weighting correcting coefficient,  =0.04 is the parameter from the age-weighting function,
=0.04 is the parameter from the age-weighting function,  is the age of onset and
is the age of onset and  is the duration of disability or time lost due to premature mortality.
is the duration of disability or time lost due to premature mortality.
Results
Submodel 1: serological evidence for EV-A71 infection rate
Among the seven contesting models, model 7 with an unconstrained initial rate of infection and a decreasing rate of infection that reaches 0 at time T has the best fit to the data. The model formulation is

where  represents the seropositive rate at time t, c and k are positive real numbers and
represents the seropositive rate at time t, c and k are positive real numbers and  is the rate which seropositivity increases (due to new infections).
is the rate which seropositivity increases (due to new infections).
The fitted values are c = 2.3 (95% CI 1.47 to 5.28), k = 4.79% (95% CI 1·92% to 8.07%), T = 9 years (95% CI 9 to 10), which translates to around 10% required infection rate in the first year of life, decreasing to 5% at ages 5–6, and drops to infinitesimally near 0% at around age 9 (figure 2, mid). Details of all models, their estimated parameters and the DIC can be found in online supplementary appendix A1, A2 and A3.
Submodel 2: incidence analysis within Singapore
The year effect,  , which captures the yearly variation of total HFMD incidence (figure 3, mid) has a correlation >99% with the overall number of cases of HFMD in Singapore. There is a positive slope of gradient 0.026 (95% CI 0.0003 to 0.052) indicating an increase in number of cases over time. The year effect of EV-A71 is estimated using laboratory data (figure 3, right) and does not have a significant trend with slope −0.0091 (95% CI −0.033 to 0.015). Year effects are presented in online supplementary appendix table A4.
, which captures the yearly variation of total HFMD incidence (figure 3, mid) has a correlation >99% with the overall number of cases of HFMD in Singapore. There is a positive slope of gradient 0.026 (95% CI 0.0003 to 0.052) indicating an increase in number of cases over time. The year effect of EV-A71 is estimated using laboratory data (figure 3, right) and does not have a significant trend with slope −0.0091 (95% CI −0.033 to 0.015). Year effects are presented in online supplementary appendix table A4.
The age effect  (online supplementary appendix table A5) which captures the systematic variation of incidence attributable to age is estimated from data from years 2005 to 2012 and is representative of the proportion of total incidence for each age, showing that >50% of disease incidence are due to children <4 years of age. Around 2.2%–2.9% of the population is affected by EV-A71 each year during their younger ages (1–3), but this quickly reduces to 1.2% by age 5 (figure 2, mid).
(online supplementary appendix table A5) which captures the systematic variation of incidence attributable to age is estimated from data from years 2005 to 2012 and is representative of the proportion of total incidence for each age, showing that >50% of disease incidence are due to children <4 years of age. Around 2.2%–2.9% of the population is affected by EV-A71 each year during their younger ages (1–3), but this quickly reduces to 1.2% by age 5 (figure 2, mid).
For Singapore, the required rate for new infections is much higher than the actual observed level, and the differences are due to asymptomatic infection. For the most vulnerable age group, around 70% of EV-A71 cases do not show sufficient symptoms to be identified either at presentation to their preschool or by their doctor (figure 2, right). Given the high intensity of Singapore’s notification system, this is arguably a lower bound on how much unnotified infection there is across other Asian countries.
Submodel 3: hierarchical model of disease severity
For HFMD in general (ie, without reference to the specific viral agent), the symptomatic case hospitalisation ratio is estimated to be 6% (2.8%–14.9%). Among hospitalised cases, 18.7% (6.7%–31.5%) develop CNS complications, of which 5.0% (2.9%–7.4%) were fatal. Overall, the CFR for HFMD is estimated to be 52.3 (24.4–92.7) per 100 000 symptomatic infections. Among the papers which identified EV-A71 as the pathogen, the majority recruited children seeking treatment in hospitals. Of these, 36.9% (25.9%–48%) were associated with CNS complications, of which 10.5% (4.9%–17.8%) died. In contrast, there were no discernible differences in the fatality rate of HFMD patients with CNS complications between cases with EV-A71 and all HFMD infections, possibly because most severe cases were indeed caused by EV-A71. Estimates within studies and overall are presented in figure 4 and table 1, which show a summary of all estimated severity quantities of HFMD in Asia with their associated uncertainties.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Data and results from the hierarchical model (submodel 3). Top: hand, foot and mouth disease (HFMD) severity for total HFMD. Bottom: HFMD severity for lab-tested EV-A71 cases. These were modelled in two separate hierarchical pyramid models. The median and 95% credible intervals for each individual paper are shown by the black dot and lines, respectively. All estimates at the individual level are based from a hyperparameter or a higher-level parameter. The vertices of the diamond show the median (also the red line) and 95% Bayesian credible Intervals. These represent the overall estimate for each severity index, where the estimates are linked together with a multiplicative relationship: P(D|C) = P(D|S) × P(S|H) × P(H|C). All parameters were estimated using a Bayesian hierarchical approach using Markov chain Monte Carlo. Case hospitalisation ratio estimate for EV-A71 cannot be calculated as studies on EV-A71 cases are almost performed exclusively from hospital data, and thus the lowest level is ‘hospitalised’ and not ‘cases’.
Overall disease severity of hand, foot and mouth disease (HFMD)
Disease burden
The disease burden estimated using our approach is 96 900 (40 600–259 000) DALYs per annum in eight high-endemic countries in East and Southeast Asia (estimates by country are provided in table 2). Our approach is conservative and will represent the minimum expected burden of disease. Despite the low CFR, the majority of disability comes from mortality (~99%) because deaths from those aged 1 to 3 years contribute very long disability lengths. In contrast, the disability length for mild symptomatic HFMD is estimated at 6.0 (5.8–6.2) days; hospitalisation about 8.3 (8.1–8.5) days, while HFMD with complications at (10.4–11.1) days.
Annual disability-adjusted life—year (DALY) losses in eight Asian countries/regions with 95% credible intervals (CI)
Discussion
In this study, we used a statistical modelling approach to synthesise information on HFMD from countries in East and Southeast Asia where the disease is highly prevalent. To estimate a conservative lower bound for the asymptomatic rate of EV-A71, we used case notification data from Singapore. The small, clearly demarcated jurisdiction with policies that lead to comprehensive case finding of symptomatic HFMD cases—notification being currently mandatory for physicians and childcare centres—may permit a higher fraction of symptomatic cases to be notified than other settings. Supporting evidence comes from the higher reported incidence rate of HFMD in Singapore (around 6%–14% at age 1) than in other areas (eg, about 3–5 times higher than China where the incidence is around 3% at age 1,3 despite Singapore having lower average EV-A71 seropositivity rates; figure 2, left). Under the assumption that conditions in Singapore permit all symptomatic HFMD to be detected, then the difference between the infection rate of EV-A71 and the incidence rate of EV-A71 gives an asymptomatic rate which, at 71.4% (68.3%–74.3%) for ages 1–4 (figure 2), is comparable to previous estimates.14
Such a high asymptomatic rate for HFMD has implications on estimates of R0, the basic reproduction number. A large proportion of unobserved infections imparts a downward bias on estimated infection rate parameters in compartmental models (such as susceptible-infected-removed variants) that assume all cases are symptomatic, and accounting for the high asymptomatic rate could be the key to reconciling the highly heterogeneous R0 estimates in the literature, which vary from almost unity to over 20.14 71–75 Other assumptions that may not always be justified include the assumption that the entire population of a school are susceptible before each outbreak.71 76
When performing data synthesis, there is a particular challenge in the allocation of collected information into the severity tiers defined in this study. For instance, we were concerned that the identified EV-A71 cases in the literature were subject to selection bias as it is more likely for physicians to take samples from sicker children. We therefore excluded studies that reported clinically diagnosed cases of EV-A71 because of this potential for bias, and as a result, the lowest level on the severity pyramid we could estimate for EV-A71 was ‘hospitalisations’ rather than ‘symptomatic cases’. To obtain the CFR for EV-A71, therefore, required assuming the case hospitalisation rate is the same for EV-A71 and other aetiologies (ie, 6%, 95% CI 2.8% to 14.9%, table 1). This is a lower bound estimate since EV-A71 is usually more severe than others. Under that assumption, the CFR of EV-A71 infection is at least 0.23% (0.075% to 0.67%, table 1). This estimate is lower by a factor of 7 than the 2015 systematic review of EV-A71 CFR of 1.7% (1.2% to 2.4%)77 which we attribute to a difference in denominator, with the Zhao review more in line with our estimated hospitalisation fatality rate of 3.8% (1.7% to 7.0%, table 1). Based on symptomatic CFRs, EV-A71 is less severe than the relatively mild influenza A(H1N1-2009pdm) strain, which had a symptomatic CFR ranged between 0% and 1.2% in 50 published studies reviewed in ref 78. Our other estimates, of case hospitalisation, case severity and CFRs of symptomatic HFMD, align with those from an epidemiological analysis of Chinese data,3 giving credibility to both sets of estimates.
Despite the high incidence rate of HFMD, the relative scarcity of severe symptoms and the generally short disability durations led to estimated annual DALY losses in eight high-incidence Asian countries of only 96 900 (40 500–258 400), considerably below the disability caused by upper respiratory tract infections (603 000) but comparable to dengue (100 000 in the same countries) which has low incidence in China.79 However, the disability caused by HFMD is mostly associated with years of life lost (>99%), driven by long expected remaining lifespan of children in comparison to the mild, temporary disability from acute HFMD symptoms. Overall, the years of life lost due to HFMD, 96 322 (39 911–257 613), are higher than dengue 43 762 (25 444–76 488), and upper respiratory tract infection 10 767 (8 459–13 636), because the majority of the DALY were caused by years lived with disability for the latter two diseases. These findings provide evidence to support decision-making on adoption of the EV-A71 vaccines.
The challenge in calculating the disease burden of HFMD lies in integrating and synthesising available data from decades of research into useful quantities for public health actions. In doing so, many assumptions were made. In particular, we integrated data from serological and epidemiological studies from a mixture of country-level and city-level studies across Asia to develop an overall ‘Asian’ average which summarises the severity across affected parts of the continent, which differ in economic development and healthcare systems. These differences cannot be easily adjusted using statistical methods due to low amounts of information from each individual country. Differences between and within countries, however, mean that these overall estimates may not apply to local decision-making. Second, the age-specific asymptomatic rate estimates were based on surveillance data from Singapore, which we believe has a notification system for symptomatic infections presenting at primary care or in education that is close to complete, but with room for misdiagnosis. Third, societal impacts—such as the indirect costs that result from caregivers taking time off work or other impacts of control policies80—are not measured in our disease burden estimates, and future research should seek to quantify such indirect impacts of HFMD so that the full cost effectiveness of intervention strategies can be evaluated.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
Footnotes
Handling editor Seye Abimbola
Contributors WMK conceptualised the study, developed the analytical strategy, collected data, performed the statistical analysis, interpreted the results and wrote the first draft of the report. HB contributed to obtaining of data and interpretation of the results. HL and MI-CC contributed to the analysis and interpretation of results. ARC contributed to the conceptualisation of the study, analytical strategy, interpretation of results, performed critical revisions of the report and secured funding. All authors contributed to revising the paper and approved the final version.
Funding The work was funded by Singapore’s Ministry of Health, Health Services Research grant number HSRG12MAY023, Communicable Disease Public Health Research Grant number CDPHRG12NOV021, the Singapore Population Health Improvement Centre, the Centre for Infectious Disease Epidemiology and Research and the President’s Graduate Fellowship to WMK.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Requests for data access should be directed to the corresponding author.