Article Text

Abstract
Background Most of the reduction in malaria prevalence seen in Africa since 2000 has been attributed to vector control interventions. Yet increases in the distribution and intensity of insecticide resistance and higher costs of newer insecticides pose a challenge to sustaining these gains. Thus, endemic countries face challenging decisions regarding the choice of vector control interventions.
Methods A cluster randomised trial is being carried out in Mopeia District in the Zambezia Province of Mozambique, where malaria prevalence in children under 5 is high (68% in 2015), despite continuous and campaign distribution of long-lasting insecticide-treated nets (LLINs). Study arm 1 will continue to use the standard, LLIN-based National Malaria Control Programme vector control strategy (LLINs only), while study arm 2 will receive indoor residual spraying (IRS) once a year for 2 years with a microencapsulated formulation of pirimiphos-methyl (Actellic 300 CS), in addition to the standard LLIN strategy (LLINs+IRS). Prior to the 2016 IRS implementation (the first of two IRS campaigns in this study), 146 clusters were defined and stratified per number of households. Clusters were then randomised 1:1 into the two study arms. The public health impact and cost-effectiveness of IRS intervention will be evaluated over 2 years using multiple methods: (1) monthly active malaria case detection in a cohort of 1548 total children aged 6–59 months; (2) enhanced passive surveillance at health facilities and with community health workers; (3) annual cross-sectional surveys; and (4) entomological surveillance. Prospective microcosting of the intervention and provider and societal costs will be conducted. Insecticide resistance status pattern and changes in local Anopheline populations will be included as important supportive outcomes.
Discussion By evaluating the public health impact and cost-effectiveness of IRS with a non-pyrethroid insecticide in a high-transmission setting with high LLIN ownership, it is expected that this study will provide programmatic and policy-relevant data to guide national and global vector control strategies.
Trial registration number NCT02910934.
- malaria
- cluster randomised trial
- health economics
- health policy
- medical entomology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this topic?
There is conflicting evidence on the public health impact and cost-effectiveness of combining long-lasting insecticide-treated nets (LLINs) and indoor residual spraying (IRS) for malaria control, and little information on the impact on insecticide resistance, particularly with novel IRS active ingredients.
What are the new findings?
This trial randomly assigned 43 of 86 clusters to receive IRS with Actellic 300 CS in an area with high and ongoing LLIN coverage.
Epidemiological impact is assessed through active case detection in a cohort of children under 5 residing in the core area of each cluster and through enhanced passive surveillance at each health facility in the district.
Economic outcome is marginal cost per a malaria case averted through IRS with Actellic on top of LLINs in a highly endemic area, as compared with LLINs alone.
Background
Around 80% (73%–88%) of the total reduction in malaria prevalence seen in Africa since 2000 is attributed to vector control interventions.1 However, increases in the distribution and intensity of insecticide resistance, particularly resistance to pyrethroids, in key vector populations pose a formidable challenge to sustaining these hard-won gains.2 3 In this context, malaria endemic countries face challenging decisions regarding the choice and financing of vector control interventions. Country-level decision-makers and development partners increasingly look for evidence of public health impact and cost-effectiveness of different interventions to guide investments.
The WHO recommends that endemic countries protect all those at risk of malaria with long-lasting insecticide-treated nets (LLINs) or, where appropriate, indoor residual spraying (IRS).4 The WHO guidance on combining IRS and LLINs states that deploying IRS with a non-pyrethroid insecticide in an area with known insecticide resistance should be done only as part of an insecticide resistance management strategy.4 This guidance is largely based on data available in March 2014 from cluster randomised trials5–8 (see table 1 for all cluster randomised trials available to date). These studies, conducted in different transmission settings, gave inconsistent evidence and did not directly assess the cost or cost-effectiveness of the interventions. These findings highlight the question of whether or not the impact of IRS in addition to LLINS is related to transmission intensity.
Cluster randomised trials assessing the combination of IRS and LLIN with results available to date
Studies with alternative designs suggest but fail to clearly demonstrate an incremental benefit in the combined use of IRS and LLINs. Hamel et al 9 conducted a non-randomised prospective trial in a high-transmission area in Kenya using pyrethroids for IRS. This study found a marked decrease in malaria incidence in the IRS and LLIN arms. Experimental hut trials have also given inconsistent results: in Tanzania two studies using different net brands and IRS products found little benefit of adding IRS once good LLIN coverage was achieved.10 11 In Benin, however, Ngufor et al,12 using a similar design, showed that IRS with a non-pyrethroid provided additional levels of transmission control and personal protection against pyrethroid-resistant mosquitoes. A trial is currently ongoing in Ethiopia assessing IRS with carbamate in addition to LLINs in an area of seasonal transmission and relatively low prevalence.13
Additionally, a meta-analysis including data from 17 countries found the IRS–LLINs combination beneficial in terms of reducing parasitaemia in areas of medium or high transmission across sub-Saharan Africa.14
This study in Mozambique will provide detailed information on the impact (infection burden and insecticide resistance) and cost-effectiveness of adding IRS with an extended release formulation of the organophosphate insecticide pirimiphos-methyl (Actellic 300 CS, Syngenta AG, Basel, Switzerland) in a high-transmission area with high LLIN access before and after an LLIN campaign. This information will be disseminated to the Programa Nacional de Controlo da Malaria (NMCP) as well as to local and international stakeholders and decision makers to inform policy recommendations and choices regarding the combination of vector control strategies.
Primary research question
In an area with high malaria endemicity and high LLIN access, what is the incremental benefit of IRS on malaria incidence and at what level of cost-effectiveness?
Methods
Study setting
Mopeia is a district in Zambezia, one of the most impoverished provinces in Mozambique (figure 1). The projected population for 2016 was 162 188 individuals, with 31 927 (19.7%) under 5 years of age.15

Administrative map of Mopeia.
The malaria burden is high in Zambezia, with a parasite prevalence of 68% in children under 5 in 2015.16 The parasite prevalence in children 1–15 years of age in Mopeia was 47.8% (38.7%–57.1%) in 2006–2008.17 Mopeia received 175 297 LLINs through a mass campaign in 2013 and IRS in the entire district with pyrethroids in 2014.18 Pregnant women in Mopeia receive free LLINs at their first antenatal care appointment, as per national policy. All residents are targeted to receive new LLINs in mid-2017 as part of Mozambique’s national LLIN universal coverage campaign. Additional malaria control activities in the district include access to intermittent prevention of malaria in pregnancy, efforts to expand appropriate case management and behaviour change communication.19
The primary malaria vector species in Mopeia District are Anopheles gambiae s.s. and A. funestus s.s., although A. arabiensis is present as well. Data from January 2015 in the neighbouring districts of Mocuba and Morrumbala show pyrethroid resistance (52% and 34% mortality 24 hours after deltamethrin WHO tube test, and 40% and 33% mortality after lambda-cyhalothrin, respectively) in the local A. gambiae s.l. population.20
Study overview
The study is a cluster randomised trial in which all of Mopeia’s villages will continue to receive LLINs through mass campaigns and routine distribution, and half of the villages will be randomised to receive additional IRS with Actellic 300 CS.
Cluster assignment and buffering
Households and population including number of children under 5 years of age were enumerated in June–July 2016. This information was used to stratify their villages in three groups by population size. Intervention allocation was conducted during a ‘randomization ceremony’ in which village representative blindly drew spray/no-spray lots from three boxes containing the stratified village names.
A ‘fried egg’ design was chosen for the clusters.21 To avoid contamination between clusters with discordant spray status, a buffer zone of at least 1 km was defined around each core area. This was based on typical African vector flying and recapture ranges22 23 and previous similar trials.5–7 This resulted in at least 2 km separating children in discordant spray areas. Villages assigned to the same intervention status were classified as single village clusters or grouped into larger clusters when required by size. Many households were located within 1 km of the village limit but more than 2 km away from any other village. Excluding these households due to location would result in great loss of recruitment opportunities, so we constructed Delaunay triangles and subsequently create Voronoi polygons from all households’ location. Voronoi tessellation was used to ‘expand’ each village’s boundary so that it encompasses those points in which the villagers live and any point which is closer to that village than any other. This process classified every point of Mopeia as belonging to the village closest to it (figure 2). Buffers were then defined from these expanded borders. Buffering between clusters with the same intervention status was deemed unnecessary and could have limited the number of eligible participants. In order to reduce contamination, an internal buffer zone of at least 1 km was defined around each cluster’s core area, and cohort members will be selected only from core areas. Each household was added and colour-coded according to location regarding spray and buffer status (figure 3).
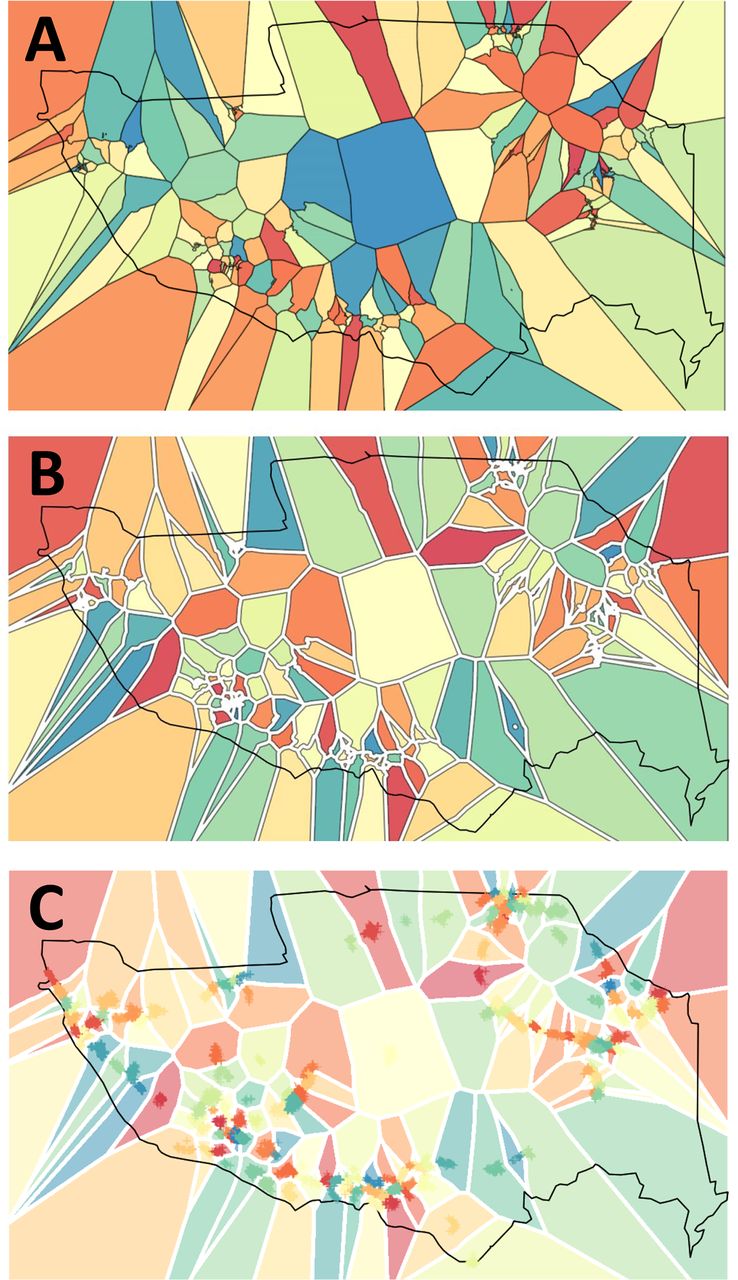
Defining cluster limits and buffers. Voronoi tessellation for cluster definition (panel A). Panel B shows the Voronoi surface with internal buffers. Panel C shows the location of every village, as well as the core and buffer areas.

Merging clusters with same status and buffering between clusters. Panel A shows the spray and no-spray regions. Panel B shows the 1-km of internal buffer added to each spray status zone. In panel C, each household was added and colour-coded according to location regarding spray and buffer status.
Intervention
The villages selected to receive the IRS intervention in 2016 will receive IRS with Actellic 300 CS once a year for 2 years according to President’s Malaria Initiative (PMI) Africa Indoor Residual Spraying (PMI/AIRS) standard operating procedures,24 in addition to standard LLIN distribution at both Antenatal Clinics (ANC) and through a 2017 mass distribution campaign. Villages selected to not receive the IRS intervention will maintain standard of care with LLINs, but will not receive IRS.
In October–November 2017 (prior to study year 2), IRS will be repeated in the same villages using the same insecticide product. Additionally, in April–July 2017 the whole district was targeted to receive LLINs from the NMCP. Information about implementation of interventions will be obtained with questionnaires during the monthly active cohort visits and during the cross-sectional surveys, including questions about wall replastering/painting and net usage. Information on quality and duration of IRS effect will be obtained through cone bioassays.
The standard of malaria care at community and health centre will remain unchanged throughout the study area, and stock levels of malaria commodities will be ensured by study partners.
Study outcomes
Primary outcomes
malaria cases averted in children 6–59 months of age at the community level by adding IRS (community incidence); the study is powered based on this outcome
cost per malaria case averted in children 6–59 months of age at the community level by adding IRS
malaria case averted in children 6–59 months of age at the health facility level by adding IRS (health facility incidence)
cost per malaria case averted in children 6–59 months of age at the health facility level by adding IRS.
Secondary outcomes
vector densities, human biting rates, sporozoite rates, indoor and outdoor feeding behaviours, prevalence and intensity of resistance to pyrethroids, and estimates of entomological inoculation rates (EIR) as measured or estimated through entomological surveillance
changes in community-based parasite prevalence
incremental impact of combining IRS with LLINs, including assessment of the impact of new nets in year 2
correlation between incidence at community and health facility levels
correlation between incidence (community and health facility) and prevalence
changes in malaria prevention methods including net use and in health-seeking behaviour.
Measurement of epidemiological impact
To determine the malaria incidence based on active case detection, a cohort of 1548, 774 children per arm, will be followed by monthly household visits. The target is to recruit 18 children from each cluster who are 6–59 months of age at time of enumeration (43 clusters per arm). During each household visit, a short questionnaire will be administered to the caretaker and a rapid diagnostic test (RDT) will be performed on the cohort child. If the child has a positive RDT, he or she will receive treatment according to the national guidelines; hence, any child who is RDT-positive at baseline will be cleared of parasitaemia for follow-up. Every time a child is treated, 10 days will be subtracted from his or her at-risk time given the half-life of artemether/lumefantrine.25
To estimate incidence rates via passive surveillance at the health facility level, a facility-based team will ensure the collection of the household location and RDT test result for each febrile patient who presents to a health facility. Enhanced passive surveillance will also include abstraction of RDT test results and treatment information from community health workers.
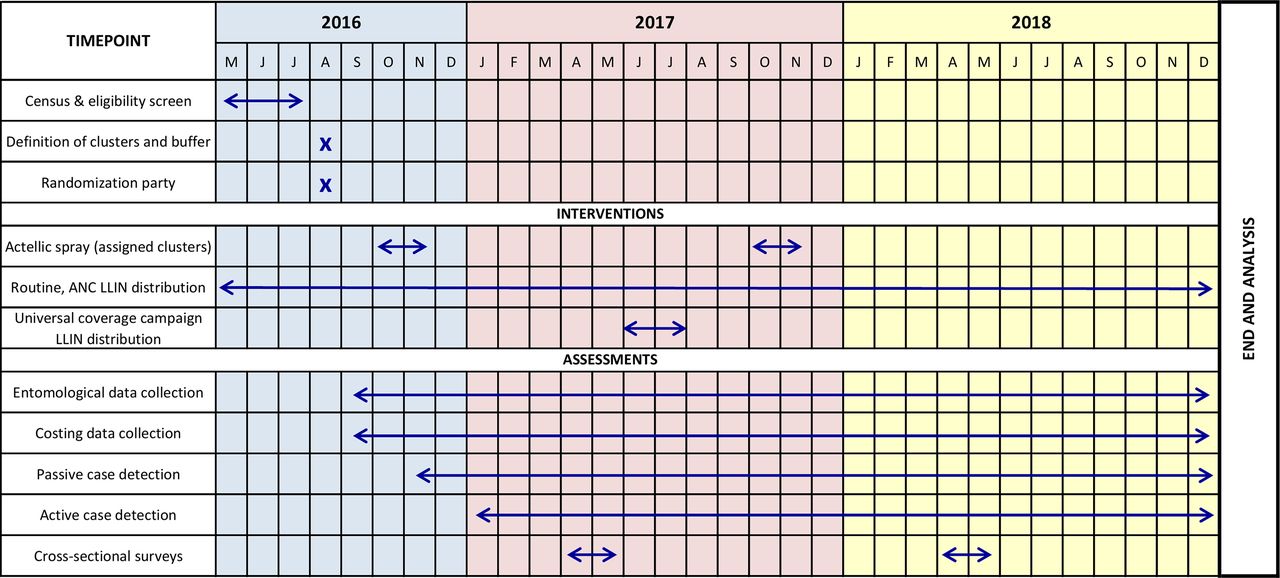
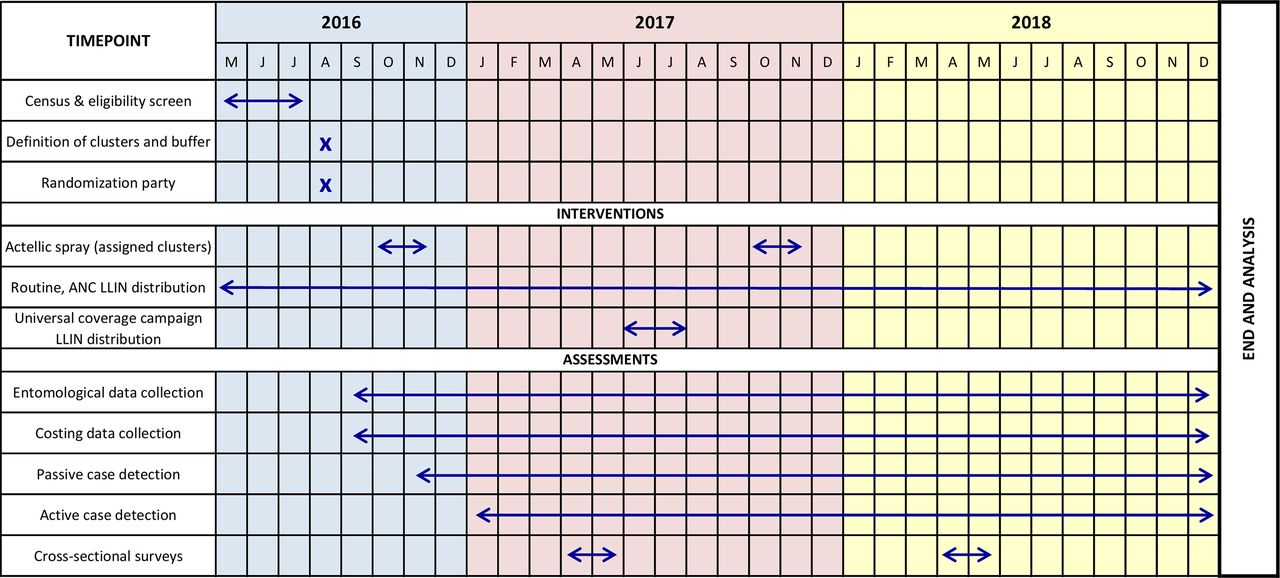
Cross-sectional studies will be carried out in April to May, at the peak of transmission season in 2017 and 2018, to estimate malaria infection prevalence and obtain additional costing and healthcare expenditure data. Figure 4 shows the Standard Protocol Items: Recommendations for Interventional Trials diagram for this study protocol.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Diagram from the Standard Protocol Items: Recommendations for Interventional Trials. LLIN, long-lasting insecticide-treated nets; ANC, antenatal clinics.
Measurement of costing outcomes
Costing data will be prospectively collected using data collection tools to determine the cost of IRS and of a case of malaria from the societal perspective.
IRS implementation costs will be recorded following an ingredient approach or microcosting26: each quantity of resource used for the programme will be multiplied by its corresponding unit cost or price. Expenditures will be inflation-adjusted and converted to US dollars, according to the official exchange rate.27
Implementation costs will be classified as financial resources needed to carry out IRS implementation,28 and economic opportunity costs, which include resources used in IRS implementation that do not necessarily involve a payment for the project but represent an opportunity cost for the society (such as car used in the IRS implementation that was not purchased and so on).
Health system costs will be obtained at the health facilities using a mixed approach: bottom-up for most of the resources used during the hospital visit or admission (tests and treatments, including the time spent by the health worker, lab and pharmacy technician) and top-down for overhead costs, in which annual operating costs of the health services will be allocated according to the proportion of the total number of services provided due to malaria in relation to all services. These IRS implementation and health service costs will be used to determine the cost from the payer’s perspective.
The societal perspective will include the aforementioned costs along with those incurred by households and individuals. Household direct costs will consist of medical and non-medical care, transportation, and others (food, telephone and others). Household indirect costs will consist of the monetisation of caregiver’s time lost (according to Mozambican minimum wage reports29 30). These costs will be collected through the cross-sectional and active case detection questionnaires.
Measurement of entomological outcomes
Entomological data, including resistance status and its changes, vector densities, sporozoite rates, and indoor/outdoor biting ratios will be collected by the PMI/AIRS project from both sprayed and non-sprayed areas using light traps and human landing catches in a subset of 10 villages, five from clusters that receive IRS and five from clusters that do not.
In each village assigned for entomological sampling, eight households will be randomly selected from the core zone for mosquito collection. Monitoring will take place on three consecutive nights every month (240 collections per month) throughout the duration of the study. Mosquito collection will be done at night using CDC light traps (CDC Miniature Light Trap, Model 512; John W Hock Company) placed indoors in proximity to humans sleeping under an untreated net at 18:00 and collected at 06:00 the following morning. Trapped Anopheline mosquitoes will be identified to species morphologically and by PCR. Salivary gland sporozoite rates will be determined by ELISA on a subset of sampled Anopheles. Molecular testing will be done to determine kdr mutation frequencies in each cluster (see below for insecticide resistance monitoring procedures).
The number of people sleeping in each collection room will be recorded and used to estimate the number of mosquitoes collected per person-time. This value will be multiplied by the observed salivary gland sporozoite rates to provide rough estimates of the EIR in different clusters and across study arms.31 Additionally, in order to better estimate the human biting rates and to estimate indoor:outdoor biting ratios, all-night human landing collections will be carried out for three consecutive nights per month at four houses from each study arm distributed in four clusters.32
The level of vector resistance to various insecticides including that on LLINs distributed in 2017 and Actellic will be monitored annually. Vector larvae and adults will be collected from representative breeding sites and households in both IRS and non-IRS areas, and the larvae will be reared to adults in the insectary for subsequent testing in WHO tube bioassays. In 2017 and 2018, at least the following insecticides will be tested using the WHO tube test: deltamethrin 0.05%, permethrin (0.75%), bendiocarb (0.1%), alpha-cypermethrin (0.05%), pirimiphos-methyl (0.25%) and DDT (4%). If resistance is detected with the WHO procedure, insecticide resistance intensity assays will be conducted based on the standard procedures of the CDC bottle assays. As described in the intervention section, cone bioassays will be used to evaluate quality of spraying and to monitor the decline of insecticide efficacy after spraying.
Sample sizes and power considerations
Power and sample size calculations conducted using the Hayes and Bennett formula33 show that 42 clusters of 12 children would provide 80% power to detect a 30% reduction in the incidence at the community level from an estimated baseline of 700/1000 children-year17 at a 5% significance level. The intercluster correlation used is 0.5 given the expected heterogeneity in transmission and the presence of displaced populations. To minimise the effect of within-family clustering, efforts will be made to avoid enrolling more than only one child per household. Number and size of clusters were increased to 43 clusters of 12 children to allow for potential loss to follow-up.
Each of the cross-sectional surveys will include an independent sample of 770 individuals, 385 children 6–71 months of age and 385 individuals 60 months and over. The sample size calculations aim at a 5% precision and have been done using estimated populations of 24 000 children 6–71 months of age and 128 000 children 60 months and over, and estimated point prevalence of 54% and 50%, respectively.
Allocation concealment and blinding
The nature of the implementation in villages makes blinding to spray status impossible to the teams collecting incidence data at the community level. Acknowledging this as an inherent limitation, IRS implementation is not concealed, yet workers doing the active case detection will not be directly informed about the spray status of the clusters they visit.
Analysis will be performed by a statistician blinded to the spray status of the clusters.
Statistical methods
Primary analysis will be conducted based on intention to treat. Analysis of incidence data will be independent and based on cluster IRS allocation, regardless of household refusal/acceptance of spray. To address the primary outcome, incidence between spray and no-spray clusters will be compared with a negative binomial regression model using generalised estimating equations that take into account the cluster design effect. Additional per-protocol analysis will be adjusted by net usage, net integrity and washes, as well as ecological, sociological and economic variables in the active cohort.
The cost-effectiveness ratios associated with IRS implementation will be expressed as cost per (1) episodes or (2) deaths averted. Following a societal perspective, the incremental cost-effectiveness ratios (ICERs) can be expressed as the following:

The threshold level of the ICERs used to define the implementation of IRS as cost-effective will be standard levels defined by the World Bank and by the WHO.34 35 ICERs will also be compared with other malaria interventions in the existing literature.36 37
To allow for uncertainty, all model parameters will be included as probability distributions rather than as point estimates, and probabilistic sensitivity analysis will be subsequently undertaken. Kullback-Laibler test for divergence between distribution will be used to fit parameter distribution obtained through data collected in the study. For those input parameters where no data are available, ranges will be derived from published literature. Monte-Carlo simulations of the probabilistic sensitivity analysis will be used to compute ICER SE and the corresponding CI.
Discussion
This study aims at providing Ministries of Health and funding partners with additional evidence regarding the public health impact and cost-effectiveness of combining the most effective vector control tools currently available, LLINs and IRS.
Some of the limitations of this study include the lack of a clear epidemiological characterisation at baseline and the 2-year follow-up period that involves practicalities regarding sample size and potential loss to follow up (LTFU) (see below).
Despite these limitations, this study has many strengths that will generate critical information on the cost-effectiveness and entomological impact of using a next-generation IRS product in a context with very high malaria transmission, existent pyrethroid resistance and high coverage of LLINs. These include random allocation of IRS to clearly defined clusters with ample buffer zones, which should contribute to the reliability of the results. The population was closely involved in cluster allocation and has responded well during pre-enrolment community mobilisation.
This study also includes rigorous, multiple methods for determining intervention impact using both active and passive surveillance, entomological data and cross-sectional surveys. Sample size calculations took into account potential LTFU in every cluster and potential loss of up to two full clusters. Lastly, this study will prospectively cost both IRS implementation and the payer and societal cost of malaria in order to determine the cost-effectiveness of the intervention. These data are expected to provide much-needed information to guide future vector control decisions in Mozambique and in similar settings.
References
Footnotes
CJC, SA, RZ, MR and FS contributed equally.
Handling editor Alberto L Garcia-Basteiro
Contributors BC, RZ, AS, MR, CLC, JW and FS conceived the study. CJC, CLC, MR, JW and JB planned the cluster design and calculated the sample size. CJC, SA, JW, RZ, KV, MR and FS wrote the first draft of the protocol. CJC, SA, JW, RZ, MR and FS wrote the data collection and informed consent forms. BC, EM and HK contributed to study design and assessed emerging issues during planning and initial implementation. SA planned and wrote the costing methods. CS designed and implemented the census. KV, LL and CF planned and wrote the entomological methods and are responsible for entomological data collection. JB delineated and randomised the clusters and produced the maps and implementation lists. All authors contributed to, read and approved the final manuscript.
Funding Funding for this study was provided by PATH, through a grant from UNITAID primed by the Innovative Vector Control Consortium (IVCC), and by USAID through the US President’s Malaria Initiative. CJC is supported by a Ramón Areces Fellowship. JB is supported by an Erasmus Mundus Joint Doctorate Fellowship, Specific Grant Agreement 2016-1346. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This protocol has been approved by the Institutional Review Board of the CISM (CIBS-CISM), the National Bioethical Committee (Comité Nacional de bioética para a Saúde de Moçambique (CNBS), the PMI Operational Research Committee and PATH’s Research Ethics Committee (REC). This study was reviewed by the Centers for Disease Control and Prevention (CDC) and determined to be human subjects research with non-engagement by CDC staff.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The full protocol is available from the corresponding author upon reasonable request.
Author note Some members of the sponsor institutions participated in study design (MR, JW, RZ, AS, CLC and CF). The primary data collection, management and analysis remain the responsibility of the CISM, with other investigators contributing to secondary analysis, in coordination with CISM. Writing of the report will be a joint effort of the participating institutions.