Article Text

Abstract
The Farmácia Popular Program (FPP) launched a subsidy system in Brazil, but in coexistence with the ongoing regular governmental access to medicines (Unified Health System (SUS) dispensings) mechanisms, causing overlaps in terms of financing and target population. This characteristic is quite different from most countries with medicines cost-sharing schemes. This paper aims to analyse the FPP under a health systems perspective considering the different health system levels. We analysed the findings from the study ‘Impact of consecutive subsidies policies on access to and use of medicines in Brazil – ISAUM-Br’, designed with the objective of describing and evaluating the impact of the government medicines subsidy policies implemented between 2004 and 2011. Patient share of copayment increased with the implementation of the intervention, which decreased the reference price and decreased with SNP (Saúde Não Tem Preço; zero copayment for patients). There was an increased number of FPP dispensations over time, but SUS dispensings remained the most important source for medicines, especially for hypertension and diabetes. FPP allowed the establishment of a well-designed pharmaceutical information system in the country. Despite the improvement on control mechanism, fraud remained a problem. There were important effects on the pharmaceutical market and sales of generic medicines. FPP has proven to be a very important policy for promoting access to medicines for hypertension and diabetes in Brazil. Examining this policy with a health system perspective has allowed us to highlight many of its important consequences, including for the first time a broad and consistent information system on access to medicines in the country.
- pharmaceutical policies
- health systems
- cost sharing
- medicines
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial IGO License (CC BY-NC 3.0 IGO), which permits use, distribution,and reproduction for non-commercial purposes in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organization or products. The use of the WHO logo is not permitted. This notice should be preserved along with the article’s original URL. See: https://creativecommons.org/licenses/by-nc/3.0/igo
Statistics from Altmetric.com
Key questions
What is already known about this topic?
Previous studies signalised the increase on access to medicines based on the increase of users and sales.
Most of the previous studies used weak designs or focused on small settings.
What are the new findings?
Farmácia Popular Program (FPP) interventions showed a relevant effect on the pharmaceutical market in Brazil.
There is an overlap in target populations between the two models of governmental medicines provision.
Individual dispensing cost in FPP is much higher than in Unified Health System (SUS) facilities, despite a higher coverage of the second.
Recommendations for policy
FPP patient volume continues to grow and treatment costs per capita remain higher than in SUS; thus, system efficiency and sustainability are important future concerns.
Since transparency and accountability are important principles in health management in Brazil, our results signalise important information for monitoring the programme and improving accountability.
Introduction
The Brazilian Constitution states health as a citizen’s right and a state duty.1 Integral access to medicines (ATM) is a right clearly stated in the law (Law 8080/90), embodying this as an inalienable part of the Unified Health System (SUS).
Government subsidy policies for essential medicines, hereinafter called Farmácia Popular Program (FPP), can be organised into four periods, marked by important policy interventions. The FPP was implemented in 2004 in some publicly owned facilities. This programme was called ‘Programa Farmácia Popular do Brasil’ (Brazilian Popular Pharmacy Program), here called FPG-public. In 2006, the Ministry of Health (MoH) expanded the subsidised access programme to private pharmacies, initiating the first phase of ‘Aqui tem Farmácia Popular’ (AFP-private1). In 2009, this strategy entered its second phase after important changes in programme management and the reference price (RP) amounts reimbursed (AFP-private2). Finally, in 2011, under the name ‘Health has no price’ (‘Saúde não tem preço’—SNP-free), medicines for hypertension (HTN) and diabetes (DM), and in 2012 also for asthma, were made free to patients in both public and private pharmacies2 3 (figure 1).

Time line of the ‘Farmácia Popular’ Program (Brazil, 2004–2013). AFP, Aqui tem Farmácia Popular; DM, diabetes; FPG, Programa Farmácia Popular do Brasil; HTN, hypertension; SNP, Saúde Não Tem Preço.
The FPP launched this subsidy system in the country, in parallel with the ongoing SUS ATM mechanisms, causing several overlaps. FPP is an important as well as peculiar innovation in Brazilian public medicines financing. Previous government financing models did not include patient copayments, with medicines being provided free of charge in public healthcare facilities. National policy stakeholders have long argued the advantages and disadvantages of introducing patient copayments, in face of other ATM initiatives. To understand the extent to which FPP has achieved its goals of improving ATM for its target population and contributing to better health status, it is important to understand and connect the existing empirical evidence that can enlighten this debate.
Medicines and other health technologies are an important component of health systems.4 5 They mobilise health, political, industrial and economical interests,6 and there are many intersectoral interfaces.7 To enhance their contribution to good health outcomes and minimise hazards, it is also important to maintain adequate pharmaceutical services.8 9 As a consequence, medicine policies strongly affect and are affected by health and other relevant sectoral policies, for example, industrial and taxing policies.
System thinking enables us to understand the complexity involved in achieving better health outcomes. There are different approaches to embodying system thinking, including developing sophisticated mathematical models.10 Despite the importance of medicines and pharmaceutical services in health systems, system thinking approaches are still new in this field.11 In Brazil the interrelation among healthcare, innovation, industry and market has been widely discussed, constituting a focus for policy study known as the ‘health economic industrial complex’,12 although industrial and market issues are more at the core. Discussions that seek to understand the different interfaces of a pharmaceutical policy at distinct levels of the health system are still rare. Bigdeli et al13 offer an organising framework for structuring such analysis.
This paper aims to analyse the FPP under a health systems perspective considering the different health system levels.
We use findings from the study ‘Impact of consecutive subsidies policies on access to and use of medicines in Brazil – ISAUM-Br’,14 designed with the objective of describing and evaluating the impact of the government medicines subsidy policies implemented between 2004 and 2011. This study comprised two different approaches: literature review and longitudinal quantitative analyses, always using national-level databases, both addressing the period from 2002 to 2013. Some data sets cover different periods, so the time frame addressed may be different for some analysis. The first approach reviewed the national legislation on the FPP, scientific publications in which the programme was analysed, and grey literature such as audit reports and technical briefings, among others. The results of the literature review were used to describe the programme in terms of health financing mechanisms, programme governance and transparency, and the political context of implementation over time, and to identify national debates around the FPP both in political and in the scientific arenas.
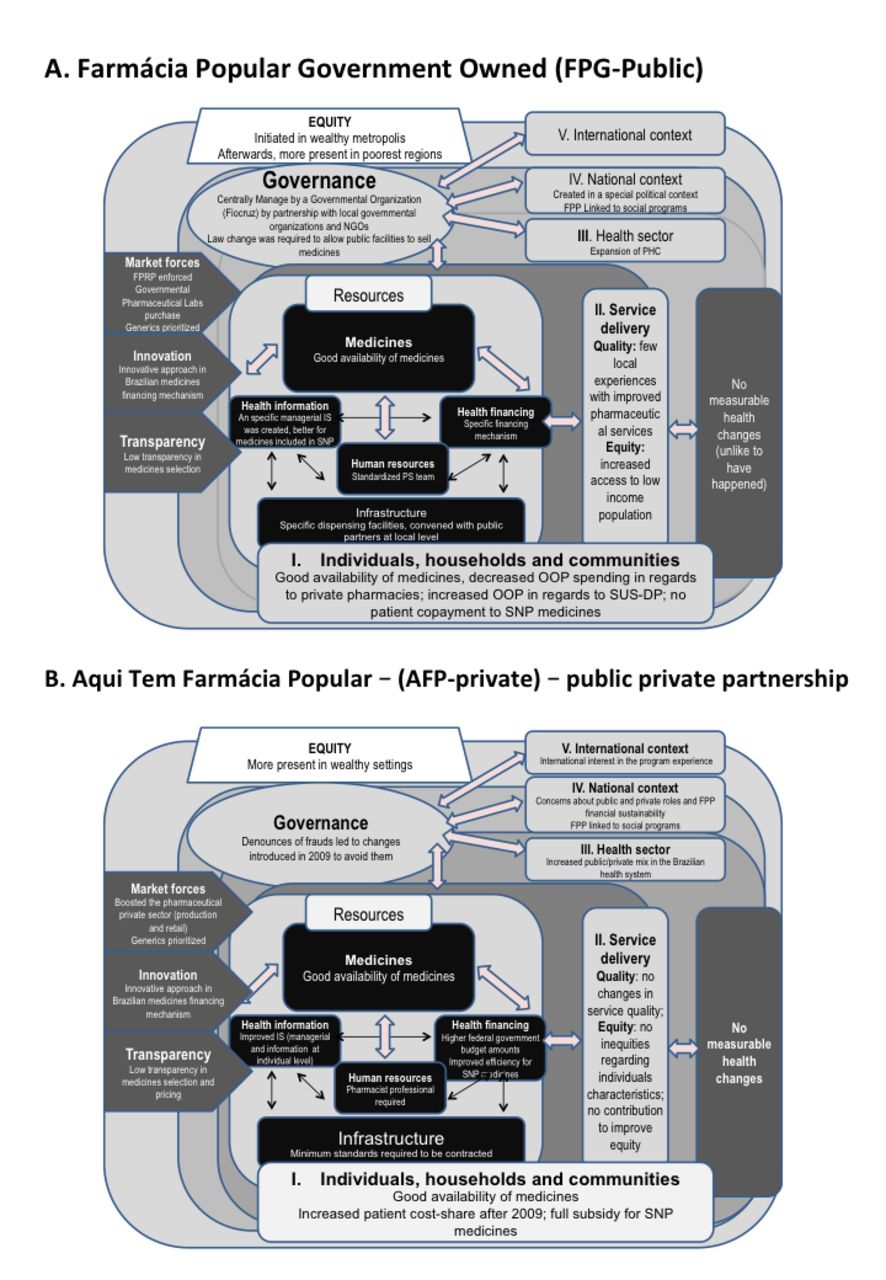
After a general presentation of key FPP characteristics, the health system levels—(1) individual and community levels, (2) service delivery level, (3) health sector level, and (4) national and (5) international levels—are used, based on Bigdeli et al,13 as a framework to organise our analysis of the effects of FP medicines subsidy programme, as summarised in figure 2 and table 1. It is followed by our integrated analysis based on international literature and wrapped up in a conclusion statement.

Main effects of Farmácia Popular, both arms - (A) Farmacia Popular Government Owned and (B) Aqui tem Farmácia Popular, by health system level (Brazil, 2004–2013). FPG, Programa Farmácia do Brasil - Rede Própria (Governmental Farmacia Popular); FPP, Farmácia Popular Program; NGO, non-governmental organisation; OOP, out-of-pocket payment; PHC, Primary Health Care; PS, pharmaceutical services; SNP, Saúde Não Tem Preço (health has no price); SUS-DP, Unified Health System dispensing facilities.
Farmácia Popular Program in a health system perspective (Brazil, 2002–2013)
General overview of the FPP
The MoH and the Oswaldo Cruz Foundation (Fiocruz) jointly managed FPG-public, created in 2004. Management responsibilities, infrastructure, financing and maintenance are shared through an agreement among the MoH and states, municipalities or universities. Fiocruz was responsible for procurement, storage, trading and dispensing of medicines. Point-of-sale stocks were centrally controlled by a computerised system. Medicines were sold without profit in a subsidy scheme, with prices kept low through bulk procurement. All revenues generated by the programme were reinvested in its own management.15
In 2006, the programme expanded through a partnership with private pharmacies, a move envisioned from the onset of the programme. A working group composed of MoH members and the Brazilian Federation of the Pharmaceutical Industry designed the expansion.16
Regarding governance, as an element of Brazil’s general health policy, FPP is subject to a broad set of rules, detailed in MoH ordinances, following principles of accountability, transparency and social participation.1 17 Audit bodies such as the Brazilian Federal Court of Accounts (TCU) monitor performance to ensure that those principles were achieved.
Based on an inspection performed on AFP-private in 2010, TCU reported18 very weak internal control; for example, medicines were dispensed without prescriptions, the dispensing receipt had missing information and there is no monitoring to detect fraud.
Measures introduced by the MoH19 after the TCU’s report led to the design of the AFP-private2 and aimed at strengthening state control. These measures were however considered insufficient, and other accountability procedures were suggested through database linkages (identifying recipients of fraudulent dispensing, overprescription by the same physician, users living outside catchment area and so on).
There are no standards on the minimum or maximum number of pharmacies associated with the programme, and no criteria such as geographical location nor demographic density were defined. The only limit on the annual number of new pharmacies was the budgetary target. Accreditation required compliance with health, labour and commercial regulations, having a pharmacist in charge, capacity to issue electronic invoices and receipts, web connection, and staff trained to carry out AFP-private rules and procedures.
In AFP-private, the MoH established an RP for each medicine, based on active ingredients and presentation. When the selling price is higher than RP, the MoH pays 90% of the RP and the patient pays the remaining value. When the selling price is equal or lower than RP, the MoH pays 90% of the selling price and the patient 10%.
There are no restrictions on users in FPP and the amount dispensed must follow the prescribed dosage and treatment duration.
FPP targets medicines that are used to treat the most prevalent diseases in outpatient care20 (37 therapeutic classes and 131 medicines for FPG-public, 7 therapeutic classes and 33 medicines for AFP-private, and 3 therapeutic groups and 25 medicines for SNP; see online supplementary appendix). Prescriptions are valid for 120 days, except for oral contraceptives, which are valid for 360 days. Dispensing occurs on a monthly basis.
Supplementary file 1
Individual and community levels
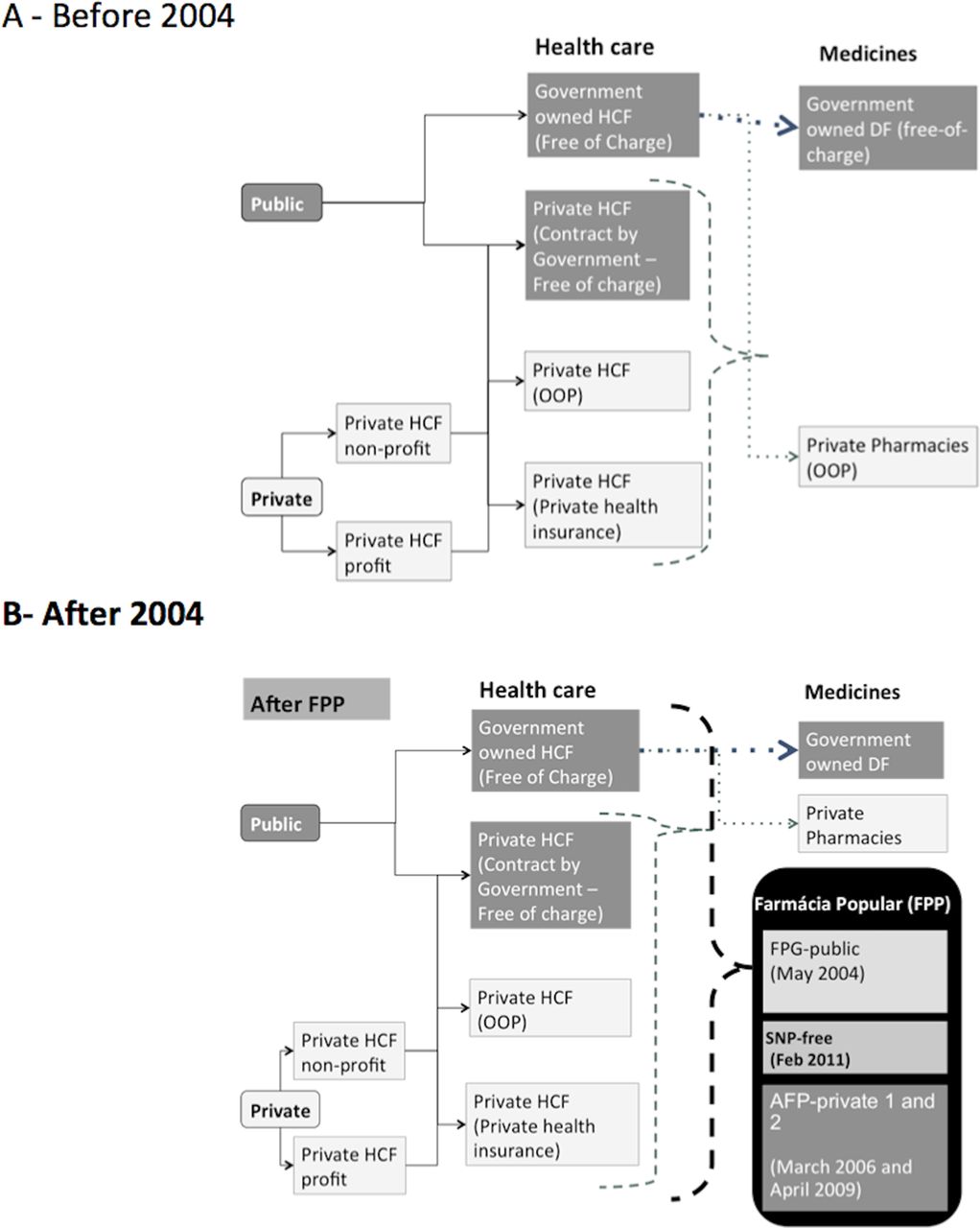
Farmácia Popular targeted primarily low-income population using private healthcare services,21 since SUS users have access to medicines through public health facilities free of charge. The rationale was high burden of expenditures for low-income households, as Brazil’s private health insurance generally does not include coverage of outpatient medicines (figure 2). Patients who received healthcare from both public and private services could obtain their medicines in FPP (figure 3).

Access to healthcare and medicines mechanisms in Brazil before (A) and after (B) Farmácia Popular Program (FPP). HCF, Health Care Facility; DF, Dispensing Facility; FPP, Farmácia Popular Program; FPG, Programa Farmácia do Brasil - Rede Própria (Governmental Farmacia Popular); SNP-free, Saúde Não Tem Preço (health has no price); AFP-private 1 and 2= Aqui Tem Farmácia Popular (Farmacia Popular is available Here phase 1 and 2).
It was found more in the beginning of FPP (2007) that about half of prescriptions originated from SUS (47.9%) and from the private sector (52.1%).21 In ISAUM-Br, when the 2009–2013 period was analysed, a lower proportion of prescriptions from the public sector (25%–35%) was found. Since people having healthcare in the public sector are allowed to fill their prescriptions in public dispensing facilities, this means a shift of FPP to its target population a long time and suggests a better performance on the availability of medicines in the public sector. Since both healthcare and medicines provisions are free of charge in SUS, competing explanations are unlikely.
We found two studies in the period covered by the literature review reporting on patients’ perspective on medicine availability, one addressing FPG-public22 and the other the AFP-private.23 Both studies found that patients were satisfied with the availability of medicines in FPP; however, some reported dissatisfaction with availability, which was related to lack of knowledge on reference medicines list. A higher level of user satisfaction was found in FPP, both in FPG-public22 and AFP-private.23
Besides geographical aspects, probably linked to wealthy regions, no other equity issues were observed in ISAUM-Br, although only gender and age were analysed.
The FPG-public represented a more expensive mechanism to guarantee access compared with the SUS dispensing facilities. However, it represents a more affordable mechanism than the private retail pharmacies for the target population, since prescriptions from the private system are not filled in SUS dispensing facilities.
In AFP-private2, ISAUM-Br found that patients’ share of copayment increased after alterations in medicines’ RP, and a larger share of the cost was shifted to patients. Prior to the change in RP, patients’ share of the cost for generics was around 10%, while for originators this percentage varied widely (eg, 65% for captopril). After the policy change, the share of cost for patients varied from 10% to 35% for generics and from 45% to 80% for originators medicines. After SNP-free, affordability was not an issue anymore for the covered medicines, which started to be fully subsidised.
ISAUM-Br estimated that FPP covered around 10% of patients with HTN and 13% of patients with DM by 2012, based on the prevalence data from VIGITELi (an annual telephone survey applied in all Brazilian state capitals). The annual coverage was estimated based on the average number of patients who obtained two or more dispensing per year from the programme divided by the estimated number of patients in need of treatment.
There was a marked increase in patient participation in the programme over time, especially in AFP-private. In FPG-public, the number of monthly dispensing increased from 300 000 in 2004 to 900 000 in 2013. Meanwhile, in AFP-private, the monthly number of dispensing for DM and HTN medicines in 2008 was 24 500 000 and 69 400 000, respectively. After administrative changes in 2009 (AFP-private2), there was a decrease in dispensing of 54.5% for DM and 60% for HTN medicines. When the SNP was implemented, the number of monthly dispensings increased dramatically, reaching 76 200 000 for DM and 244 700 000 for HTN medicines after 1 year (February 2012).
ISAUM-Br14 also calculated the proportion of days covered (PDC) by medicines dispensed from the FPP. PDC is a widely used measure for adherence to treatment. In this study, it was used to refer to consistency of dispensing from the FPP, since there are other unobserved sources of medicines available to patients. There were data to measure PDC only during the AFP-private phase of the FPP. During 2008, the PDC for HTN and DM medicines varied from 50% to 75% depending on the medicine. After the cost share increase in 2009 (AFP-private2), the PDC decreased to approximately 60%. With the implementation of the full subsidy programme, PDC increased for all covered medicines, reaching an average of 80% for all medicines analysed.
Service delivery
For the first time under FPP, Brazil had a national pharmacy programme information system comparable with those found in high-income countries. In AFP-private, the sales authorisation system regulates the maximum dispensing amounts according to therapeutic protocols and links purchase to the individual taxpayer identification number (Cadastro de Pessoa Física—CPF). The link to the CPF allows the system to verify its validity and prevent the same patient acquiring medicines repeatedly in different AFP outlets. These control mechanisms are an important fraud reduction strategy. Additionally, the system allows the programme to monitor the regularity of medicines dispensing to patients. Use of CPF allows linkage to other national databases and calculation of patient-level indicators of adherence linked to treatment and health outcomes. However, this linkage is only valid for medicines dispensed under the AFP-private and SNP, and not the FPG-public medicines or SUS. Thus, duplication of dispensing between SUS and AFP-private is possible.
Availability of medicines was found between 90%24 and 100%.25 However, these studies took place in AFP-private1, with data from 200725 and 2008/2009,24 and the latter covered only one Brazilian state.
No evidence was found of any impact of AFP-private on the quality of private pharmaceutical services. On the other hand, FPG-public established national performance standards in governmental pharmaceutical services. FPG-public in a north-eastern municipality was found as enabling good pharmaceutical care.26 Indeed, positive outcomes were observed among hypertensive27 and elderly28 patients receiving pharmaceutical care from FPP in two different municipalities. It was also found29 that FPG-public patients were more likely to receive information in relation to private pharmacies and that the regulations on dispensing were followed for all patients. It is important to highlight that these studies were conducted in a university-owned FPG-public pharmacy, with specific characteristics that might influence results.
FPP clearly influenced prescribing behaviour, such as the shift from captopril and enalapril to losartan after its adoption in 2010, or increase in the use of generics after SNP.
A growth in the density of FPP facilities coincided with the phases of the programme. In FPG-public, there was a sharp increase in the numbers of participating pharmacies after 2006, stabilising in 2009. In AFP-private, facility density increased substantially after AFP-private2 (2009) and it continued to grow throughout 2011.
There was an increase in FPP coverage in most regions between 2006 (when the private pharmacy component started) and 2013; however, participating pharmacies remained unequally distributed across geographical regions. FPG-public was more present in the north and north-east regions, which are poorer areas with greater need for access to medicines and healthcare. Meanwhile, AFP-private pharmacies were more concentrated in wealthy areas in the south and south-east, following the distribution of the private retail pharmacies in the country.
Minor changes were observed in hospital admissions for HTN and DM following the FP policies.14 We believe the small reductions observed are an effect of multifactorial policies implemented for chronic diseases along the period analysed where FPP is a component.
Health sector
Medicines covered by FPP had higher market share for HTN and DM for all FPP phases. In AFP-private2, market share of losartan increased, while market share of captopril and enalapril decreased, suggesting a shift in the prescription pattern towards losartan, mainly after SNP. Among the sulfonylureas, glibenclamide achieved the highest market share (60%) after the SNP intervention. Metformin had 100% of biguanides’ market share throughout the study period.
FPP reinforced the objectives of Brazil’s generics policy; within the FP programme, generic medicines had the highest sales volume and market share for antihypertensive and hypoglycemic medicines (55% and 75%, respectively) by December 2012. Since generics are typically the option with the lowest cost in a class, this might explain the increasing sales volume and decreasing cost per capita after SNP-free, when the government paid a fixed price per class to the retail pharmacy.
The overall cost per treatment to the MoH declined by 23% for both diseases, showing that FPP made HTN and DM treatment more affordable to the government, mainly after SNP (2011). Data on volume, price and expenditure within FPG-public are limited to 2011 and 2012 (figure 4). During this period, unit prices in the FPG-public were six (captopril/atenolol) to eight (propranolol/hydrochlorothiazide) times lower than AFP-private, depending on the medicine. However, FPG-public accounts for only about 10% of the volume for HTN and DM medicines in FPP (table 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ministry of Health monthly total expenditure per person and out-of-pocket on hypertension (A) and diabetes (B) treatment —Aqui tem Farmácia Popular (AFP) (Brazil, 2006–2012). MoH, Ministry of Health; SNP, Saúde Não Tem Preço.
Total year volume in units, proportion of volume in AFP-private and FPG-public, and unit price (local currency) by medicine for hypertension and diabetes treatment, Farmácia Popular 2011–2012
Despite lower MoH expenditure per treatment, in light of increased utilisation, it is important to consider the financial sustainability of the programme. Population coverage for HTN and DM was around 13% by 2012 within the FPP; sustainability could be hampered if more people prefer FPP as their source for medicines. Since HTN and DM medicines are free of charge in FPP and in SUS, any increase on ATM barriers in SUS may drain patients to FPP.
SUS is a decentralised health system; nevertheless, FPP is a centralised programme in all aspects. All decisions are made by the MoH with little or no discussion involving SUS collegiate bodies, representing challenges in governance to overcome.
Information on FPP is accessible through the internet, mainly in the Strategic Management Support Room (Sala de Apoio a Gestão Estratégica—SAGE,ii an MoH situation room). However, FPP data are not as easy to obtain as other government programmes.
Payments to pharmaceutical retail establishments are recorded as Health National Funds (Fundo Nacional de Saúde) direct transfers. This system identifies which federation units have the highest number of pharmacies and highest payment volumes. Specific medicines provided by the AFP-private and the amounts spent on each medicine are still missing from the database.
National and international context
Farmácia Popular was proposed as part of President Lula’s work plan during his first mandate. Indeed, Machado et al30 claim that ‘Farmácia Popular’ together with ‘Estratégia de Saúde da Família’ (Family Healthcare Strategy), ‘Brasil Sorridente’ (Smiling Brazil—an odontology programme) and ‘Serviços de Atendimento Móvel de Urgência’ (Mobile Urgency Care Service) were the most important policies implemented in this period.
Pernambuco, a north-eastern Brazilian state, implemented a subsidy policy for medicines in 2001, establishing the basis for the national programme and for two similar state programmes, one in Rio de Janeiro and another in Rio Grande do Norte.15 Humberto Costa, the first Minister of Health during Lula’s first term, and had been Pernambuco State’s Health Secretary, helped to elevate the state programme into a national policy.
Trevisan and Junqueira31 argue that FPP has played a role in MoH’s strategy to contain the pharmaceutical industry’s commercial deficit by encouraging the link between national production of pharmaceuticals and SUS network management. These authors state that FPP has led to increased medicines consumption among the two lowest income tiers of citizens. This has increased employment and income, and increased the number of medicines outlets targeting low-income citizens, leading to greater consumption of pharmaceuticals not covered by the FPP, mainly branded generics (called ‘similares’ in Brazil).
Some countries in Latin America have shown interest in the popular pharmacy programme, such as Peru and Ecuador. Both evaluated the FPP for increased access to medicines, and in 2013 signed cooperation for the transfer of technology in the area.32
Some integrated thoughts on Farmácia Popular
The effects of medicines cost sharing are widely discussed in the literature.33–37 In general, cost sharing has the declared intention of reducing health system costs and improving sustainability.38 The FPP however has a different objective of improving medicine access and reducing households’ financial burden. In addition, overlaps among ATM mechanisms in health systems as it occurs in Brazil with FPP and concurrent free-of-charge medicines dispensing at SUS facilities are rare; therefore, FPP represents a peculiar case.
FPP represents a special example of political agenda setting using access to medicines. First, it required strong and consolidated leadership to define priorities and achieve implementation targets.39 40 Second, implementation was enforced through important institutionalisation steps, including the introduction of the First National Conference of Medicines and Pharmaceutical Services report, signed by the Minister of Health, announcing ongoing studies for the implementation of Farmácia Popular.41 Also, the matter was discussed in the National Health Council, an important policy forum in Brazil.42 43 Unrestricted access through FPP operationalises the principle of universal access in Brazil while filling the gap left by failures in SUS free-of-charge medicines provision. However, despite the importance and magnitude of this policy, we were not able to find a publicly available implementation plan that considered budgetary impact or that forecasted the long-term number of potential users. Additionally, some stakeholders claim that it would be worthwhile to strengthen medicines provision in SUS instead of invest in another programme, because it would compete for scarce resources and managerial efforts.44
A study using data from a national primary healthcare service survey in 2012 found that the average availability of medicines was 58.5%, with better results associated with better pharmaceutical services infrastructure, including pharmacist support.45 However, user satisfaction was high for both AFP-private and FPG-public.
Prices are a central concern in FPP. Prices in FPG-public were lower than in AFP-private, and the reference medicines list in FPG-public was broader (table 1). However, the lower number and poorer coverage of FPG-public dispensing facilities2 hinder some of these advantages. The impact of AFP-private2 increased the prices paid by patients compared with the earlier policy, because of decreases in RP. Rather than lowering sales prices in response to the reductions in RP by the MoH, private pharmacies kept selling price at previous values, resulting in an increase in patient cost share. In contrast, sales prices were noticeably reduced after SNP, since there was no longer incentive for high prices because the MoH paid only the RP. With the new policy, it was possible to decrease per capita treatment costs and expenditure.
We found an average monthly FPP coverage of 10% and 13% of patients with HTN and DM, respectively. These rates are quite similar to estimates from two surveys about the same period, which found also that SUS dispensings were the main source of medicines for HTN and DM, at about 50%.46 47 However, these findings differ from a Demographic and Health Survey, which found that one-third of individuals with HTN (35.9%) and more than half of those with DM (57.4%) obtained at least one medication through FPP.48
The rapid growth in FPP utilisation and expenditures put its financial sustainability in question. FPP has no budgetary limit, since any prescription filled under the programme in private pharmacies is reimbursed by the MoH. The situation in FPP differs from that of SUS. While expenditures on primary healthcare medicines in SUS have been unchanged since 2013 for a greater number of people and a broader medicines list, expenditures in AFP-private have continued to increase, from R$35 million in 2006 to R$2.6 billion in 2016. Three studies addressing per dispensing cost comparisons between AFP-private and SUS have found that AFP-private can be a lot more costly than public dispensing at SUS facilities.23 49 50 Meanwhile, FPG-public reached only R$99 million in 2016, of which 81% represented administrative costs and 19% medicines procurement.51 FPG-public was ended by the MoH in 2017.52 The impact of its discontinuation is yet to be determined since this branch covered poorer regions in Brazil,2 which the private retails do not reach, had broader list of medicines and had an interesting model of pharmaceutical services in course, in comparison with that from AFP-private.
Despite the important advances in the information system created to implement FPP, information has become available on the internet only recently, and important measures, such as the proportion of prescriptions originated in SUS, are still not reported.
Conclusion
Farmácia Popular has proven to be a very important policy for promoting access to medicines for HTN and DM in Brazil. Examining this policy with a health system perspective has allowed us to highlight many of its important consequences, including for the first time a broad and consistent information system on access to medicines in the country, despite some problems in transparency. FPP has clear impacts on expanding the number of private market outlets participating in the programme, increasing treatment consistency for DM and HTN, reducing patient cost share, increasing market sales volume of medicines covered by FPP, and increasing the market share of generics. Since FPP patient volume continues to grow and treatment costs per capita remain greater than in SUS, system efficiency and sustainability are important future concerns.
Acknowledgments
The authors thank the Ministry of Health in Brazil for providing the data used in this study.
References
Footnotes
↵i http://tabnet.datasus.gov.br/cgi/vigitel/vigteldescr.htm, accessed on 1 March 2015.
↵ii sage.saude.gov.br.
Handling editor Seye Abimbola
Contributors ICME and LAC were in charge of study conception. ICME and MRC conducted the main statistical analysis in the source study. VLL, LAC, ADB, MB, RMS and DR-D participated in the paper conception. All authors participated in the writing of the paper and approved the submitted version.
Funding The study received research grant from the World Health Organization Alliance for Health Policy and Systems Research. ICME was supported by Conselho Nacional de Pesquisa, Brazil (CNPq) process number 202246/2012-4 and the Pyle Fellowship of Harvard Pilgrim Health Care Institute. DR-D is supported in part by the Health Delivery Systems Center for Diabetes Translational Research (HDS-CDTR) (NIDDK grant 1P30-DK092924).
Disclaimer The author(s) is(are) staff member(s) of the World Health Organization. The author(s) alone is(are) responsible for the views expressed in this publication and they do not necessarily represent the views, decisions or policies of the World Health Organization.
Competing interests None declared.
Ethics approval The Brazilian National Ethics Committee, the National School of Public Health—Fiocruz—Brazil, and the WHO ERC approved the ISAUM-Br project, which is the base of this paper.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Author note This work was conducted in collaboration with the following institutions: Department of Medicines and Pharmaceutical Services Policies, Sergio Arouca National School of Public Health, Fiocruz, Brazil; Department of Epidemiology, University of Pelotas, Brazil; Department of Pharmaceutical Services/Office of Science Technology and Strategic Resources-Ministry of Health; and the Department of Population Medicine, Harvard Medical School and Harvard Pilgrim Health Care Institute.